What Do Chaplains Do? An Introduction to Outcome-Oriented Chaplaincy
- David Fleenor
- 8 hours ago
- 9 min read

Outcome-oriented chaplaincy asks presence to become intentional, describable, and accountable without ceasing to be presence.

Ask a group of chaplains a deceptively simple question—what do chaplains actually do?—and the answers tend to fall into two camps. Some describe a way of being: being present, accompanying, holding space, a ministry of presence. Others describe things they do that make a difference: they helped someone find peace, make a decision, or reconcile with an estranged family member. Being present, versus making a difference. Both are true, and both are precious. But the quiet tension between them turns out to be one of the most important conversations in contemporary chaplaincy. It is the conversation at the heart of what has come to be called outcome-oriented chaplaincy.
What outcome-oriented chaplaincy is
Brent Peery defines outcome-oriented chaplaincy—OOC—as “a method of chaplaincy care that emphasizes achieving, describing, measuring, and improving outcomes that result from a chaplain’s work.” Many chaplains recoil at the word measuring. How can you quantify the sacred? Who can measure meaning? Peery grants the point, in part. Much of what we do is genuinely subjective and always will be; he calls it “the complex, beautiful art and mystery of the profession.” OOC does not deny that. It simply observes that a great deal of our care is also objective—observable, describable, improvable—and it turns its attention there.
The whole approach rests on three words: assessment, interventions, and outcomes. Peery subtitles his chapter “Intentional Caring,” and that is the spirit of it. OOC is not about data for its own sake. It is about caring on purpose.
Why it developed
It is tempting to dismiss OOC as chaplaincy scrambling to justify itself under healthcare reform. Peery resists that. He describes OOC as a confluence—a joining of personal, contextual, and historical streams. One of those streams is a genuine shift in paradigms. Building on John Gleason (and, behind him, Thomas Kuhn), Peery traces three eras across a century of chaplaincy. In the first, chaplaincy was a response to individual sin—helping people heal within a shared faith tradition, the pastor or rabbi at the bedside. In the second, beginning in the 1960s and built on Carl Rogers’s client-centered therapy, chaplaincy became a response to the person; this is where the “ministry of presence” was born. In the third, at the turn of this century, chaplaincy became a response to individual need—assess, intervene, attend to outcomes. Gleason described this newest paradigm arriving “uneasily, conflictually, but irresistibly.” Peery calls it “the operant paradigm for professional chaplaincy for the twenty-first century.” Notice the middle paradigm, though: the Rogerian ministry of presence never went away, and it is the root of a tension we will return to.
Peery frames the rationale as three commitments—the ABCs. Accountability is a commitment to our employers: the shift from “here is how I spent my time” to “here is the difference this made for the patient,” documented in the record and described in language the team understands. Best practice is a commitment to those we serve: the promise to pursue the most effective care the profession knows, and to keep learning what that is. Collaboration is a commitment to our fellow professionals: OOC demystifies chaplaincy so the interdisciplinary team can actually partner with us. Three commitments, three audiences.
How it works: a cycle that starts with the person
The approach grows out of the seminal work of Larry VandeCreek and Art Lucas, The Discipline for Pastoral Care Giving. Lucas arranges the three components into a cycle that always begins with the person, never with the chaplain’s agenda. We assess the person’s needs, hopes, and resources; form a working profile; name the difference we hope to help make—the desired contributing outcome; plan and provide interventions; then measure the actual outcome against what we hoped for, and reassess. The word contributing matters. We rarely produce an outcome single-handedly; we contribute alongside medicine, nursing, family, and the patient’s own resources.

Assessment is the engine. Lucas makes one move worth holding onto: do not start with needs alone. If you do, he warns, you cast the patient as “a big bag of needs” and yourself as “a big bag of resources” in a one-way repair job. Start instead with needs, hopes, and resources together. Hopes “provide energy, direction, impetus, and motivation for the future,” and naming a person’s own resources honors their strength and dignity. In practice we attend to four intertwined spheres at once—spiritual, emotional, relational, and biomedical.
The crowded field of spiritual assessment
Assessment also has a long and, frankly, crowded history. Sociologists Wendy Cadge and Julia Bandini trace the practice from its origins in chaplaincy and pastoral care—Paul Pruyser’s 1976 The Minister as Diagnostician, Anton Boisen’s narrative tradition, nurse Ruth Stoll’s 1979 guide—outward into nursing, medicine, and social work, each field coining its own acronym tools: FICA, HOPE, SPIRIT, FACT, the 7×7 model, INSPIRIT, and more. There were more than thirty tools by the 1990s, and there are more than forty today. Cadge offers a helpful ladder: a spiritual screen (a question or two at admission, which any provider can do), a spiritual history (a brief interview any team member can take), and the full spiritual assessment (the in-depth interpretation that is the chaplain’s specialty). The catch is that disciplines rarely learn from one another’s tools, so everyone reinvents the wheel. That proliferation led George Fitchett to a now-famous challenge: we “no longer need to develop new models for spiritual assessment,” but rather “a critical review of existing models and the dissemination of best practices.”
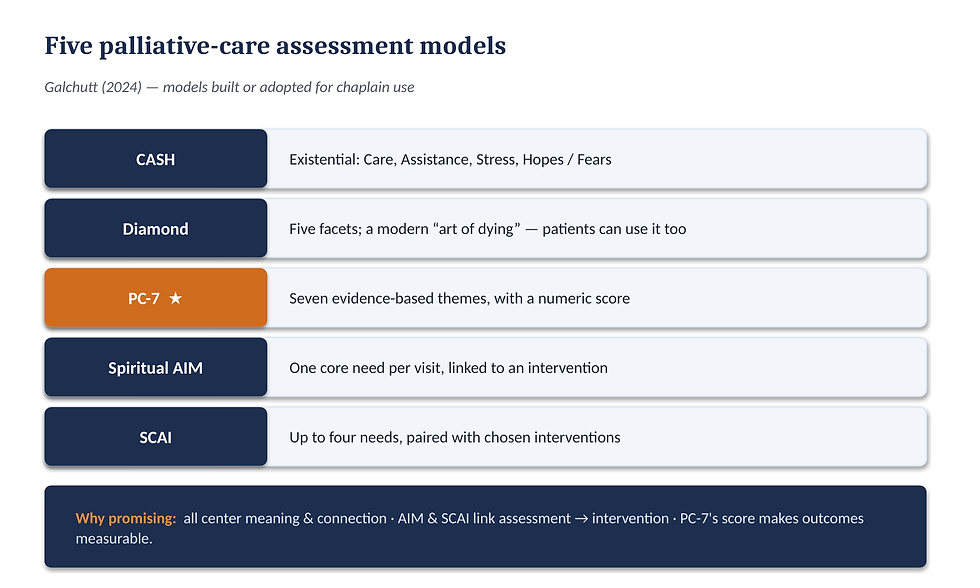
So which existing models are worth knowing? For palliative care, Paul Galchutt’s 2024 review narrows the crowded field to five built or adopted specifically for chaplains. CASH is an existential model—Care, Assistance, Stress, Hopes and Fears. The Diamond model, five facets, is a modern, non-religious reworking of the medieval “art of dying,” and can even be used by patients themselves. The PC-7 offers seven evidence-based themes and, importantly, a numeric score. Spiritual AIM identifies one primary need per visit and links it to an intervention. And SCAI assesses up to four needs and pairs them with interventions from a list. What makes these promising is that they do precisely what OOC describes: all five center meaning and connection; AIM and SCAI explicitly link assessment to intervention; and the PC-7 goes furthest—its numeric score can show patient-level change and even tell a population-level story of the difference chaplaincy makes. Fitchett’s caution still applies: use them with modesty. They are frameworks that can miss a need, always with “room for improvement.” They are maps, not cages.
Interventions: activity versus outcome
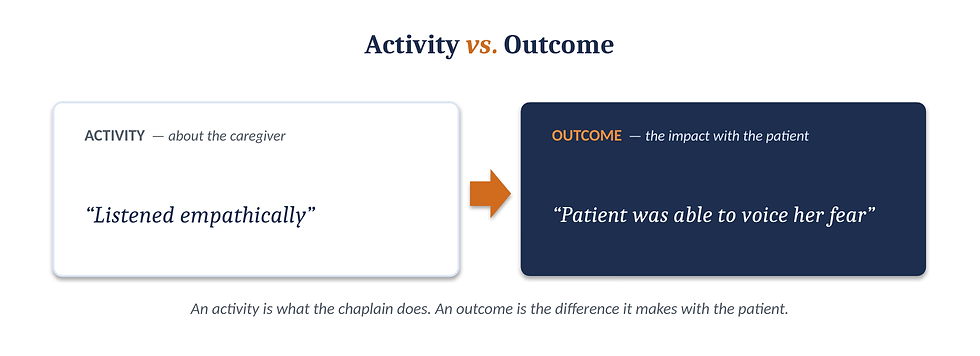
An intervention is an intentional action of the chaplain, based on the assessment and aimed at a desired outcome—“relational, intentional, and something for which we own responsibility,” in Lucas’s words. Here lies the single most important distinction in OOC: the difference between an activity and an outcome. An activity is something the chaplain does; it is about us. “Listened empathically” is an activity. An outcome is the difference that action makes with the patient; it is about them. “Patient was able to voice her fear” is an outcome. New chaplains tend to chart activities; OOC asks us to name the outcome. And here is an encouragement: many chaplains are already more skilled at intervening than at articulating what they did. Naming interventions is a learnable discipline.
The research helps. Handzo and colleagues found the most common spiritual interventions were prayer and blessing or faith affirmation, and the most common general one was empathic listening. Massey and colleagues found the most frequent were active listening, pastoral presence, demonstrating care and concern, preserving dignity and respect, and remaining open to the patient’s beliefs. A newer, wider-angle picture comes from Kelsey White, Wendy Cadge, and colleagues, whose 2026 scoping review pulled 388 distinct chaplain activities into fourteen categories. Four are “core,” each accounting for more than a tenth of what chaplains were documented doing: psycho-spiritual (counseling-type) care, spiritual assessment and support, religious rituals and services, and staff support and education. One finding is striking: our biggest category, psycho-spiritual care, is not unique to chaplains—but spiritual assessment and support is. When you name your interventions, pay special attention to the ones only you are trained to do. That is where your distinct value, and your clearest outcomes, will show up.
Outcomes: the observable results of care
Outcomes are the observable results of our care. Lucas gives two criteria. They should be sensory-based—recognizable through what we see, hear, or feel—and communicable, clear and brief enough for the team to grasp; if an outcome takes more than one sentence to state, it is not yet clear. If that language feels clinical, listen to how Lucas keeps it pastoral:
“After we have gotten to know the patient, what are we hoping for? What is our prayer for the patient?”
An outcome, in other words, is simply our prayer for the patient—made observable. The patient is able to express gratitude; articulates a hopeful story about the future; achieves calm, evidenced by reduced distress; engages effective coping. Each is about the patient’s movement, not the chaplain’s activity.
Documentation, in the era of Open Notes
None of this helps the team unless we write it down. Peery’s Memorial Hermann charting model carries a mnemonic—“run in on a prayer”: the Reason for the visit, the Interventions, the Outcomes, the Assessment, and the Plan. The note literally holds assessment, interventions, and outcomes in a form a physician, nurse, or social worker can read and use. But a recent shift changes who is reading over our shoulder. Since the 21st Century Cures Act took full effect in 2021, patients in the United States can open an app and read a chaplain’s note almost the moment it is signed. Jo Hirschmann and colleagues at Mount Sinai studied exactly this, and their recommendations are worth memorizing: write in the first person and active voice (“I prayed with Patricia,” not “A prayer was said for the patient”); make the patient, not the chaplain, the subject; use strengths-based language that names resources, not just deficits; keep it concise; and watch for language that quietly signals disbelief—quotation marks, “patient claims,” even “patient reports”—a habit many chaplains were trained into. Write as if the person you are describing will read it, because now they can. Happily, that pushes us in a very OOC-friendly direction.

The tension: process versus outcome
Not everyone welcomes this turn, and the disagreement deserves a fair hearing. The review by Annelieke Damen, Carmen Schuhmann, Carlo Leget, and George Fitchett maps it as a genuine debate between good people. On one side is process-oriented chaplaincy, which prizes presence, relationship, and being-with; its lineage runs through Freud, William James, and especially Carl Rogers, and most chaplains were trained to think in terms of process, not outcome. On the other is outcome-oriented chaplaincy, which prizes intention, description, and accountability, and speaks the shared language of healthcare so our work can be understood and integrated.
Because the process side begins with one person, he is worth a paragraph. Carl Rogers founded client-centered—or person-centered—therapy on a wager: people carry within themselves the capacity to grow, and the helper’s task is not to diagnose, direct, or fix, but to create the relational conditions in which that capacity is released. He named three core conditions: congruence or genuineness (the helper is real, not hiding behind a professional mask), unconditional positive regard (the helper accepts and prizes the person without conditions or judgment), and empathic understanding (the helper senses the other’s world from the inside and reflects it back). Rogers’s approach is non-directive, and it treats the client, not the expert, as the authority on their own experience. It is easy to see how this became “being there”: presence, not agenda; being, not doing. When critics worry about OOC, in a real sense they are defending Rogers.
The critique is serious. An outcome agenda, critics warn, can shift focus from relationship to problem-solving; the assess–intervene–measure sequence can import a medical model that pathologizes the person; standardization can flatten the unique individual, when it matters enormously who is present and how; and we risk instrumentalizing the sacred. Steve Nolan put it sharply: the question is “whether adapting to the new reality will be at the cost of distorting what we value and believe to be important about spiritual care.”
The rejoinder is that every chaplain, even the most process-oriented, already interprets a situation (assessment), responds (intervention), and hopes to deepen a relationship (an outcome). Naming those steps does not betray the work; it adds the conscious reflection that makes us accountable. The pitfalls are real but avoidable—narrative, dialogical assessment keeps the unique person, and even a transcendent horizon, in view. The most useful move is to get past either/or.
The philosopher Alasdair MacIntyre observed that every practice “aims at some good.” Chaplains, too, aim at some good—a vision of the better. Outcomes are simply those goods made concrete enough to notice. Even the ministry of presence has an agenda in that sense: a hope for the good, if never a script.
Back to the question
So, what do chaplains do? The honest answer holds both truths at once. Chaplains form real, accepting, non-anxious relationships—the enduring gift of the Rogerian tradition—and they do so intentionally, attentive to the difference their care makes for the people and teams they serve. Outcome-oriented chaplaincy does not replace presence. It asks presence to become intentional, describable, and accountable.
Further reading
Cadge, W., & Bandini, J. (2015). The evolution of spiritual assessment tools in healthcare. Society, 52(5).
Damen, A., Schuhmann, C., Leget, C., & Fitchett, G. (2020). Can outcome research respect the integrity of chaplaincy? A review of outcome studies. Journal of Health Care Chaplaincy, 26(4), 131–158.
Galchutt, P. K. (2024). Spiritual assessment models for palliative care chaplains: A narrative review. Journal of Health Care Chaplaincy.
Gleason, J. (1998). An emerging paradigm in professional chaplaincy. Chaplaincy Today, 14(2), 9–14.
Handzo, G. F., et al. (2008). What do chaplains really do? II. Interventions in the New York Chaplaincy Study. Journal of Health Care Chaplaincy, 14(1), 39–56.
Hirschmann, J., Terry, K., Van Thyn, R., & Strano, A. (2025). Chaplains’ charting in the USA in the era of “open notes.” Journal of Religion and Health.
Massey, K., et al. (2015). What do I do? Developing a taxonomy of chaplaincy activities and interventions for spiritual care in intensive care unit palliative care. BMC Palliative Care, 14, 10.
Peery, B. (2012). Outcome oriented chaplaincy: Intentional caring. In S. Roberts (Ed.), Professional Spiritual & Pastoral Care.
Rogers, C. R. (1961). On Becoming a Person. Houghton Mifflin.
VandeCreek, L., & Lucas, A. (Eds.). (2001). The Discipline for Pastoral Care Giving. Haworth Press.
White, K. B., Adjei, N., McClelland, L. E., & Cadge, W. (2026). Conceptualizing spiritual care in the U.S. through chaplain activities in research: A scoping review sub-analysis. Journal of Health Care Chaplaincy.


